1. Introduction
Transcranial direct current stimulation (tDCS) has been investigated and used for clinical purposes in neuropsychiatric conditions.1,2 It is a non-invasive brain stimulation technique that can be used to modify cortical brain activity, as well as to induce behavioural changes.3,4 The application of repeated tDCS sessions has the capacity to modify the efficiency of synaptic transmission in a relatively long-lasting manner.5
Attention deficit hyperactivity disorder is a clinical syndrome characterized by the presence of high levels of hyperactivity, impulsivity and inattentive behaviors, with onset in childhood and persistent over time, with significant clinical implications. Prevalence in children is estimated at 5%, follow-up studies suggest that approximately 50% show partial remission with persistence of certain symptoms into adulthood; prevalence is estimated at 2.5-4.3% of adults.6
Several reports have observed decreased cortical thickness and delayed maturation in frontal, temporal and parietal areas. In addition to these findings, white matter tracts have been found to be impaired in this disorder, particularly in the fronto-striato-cerebellar pathway and interhemispheric tracts, which may manifest as executive dysfunction.7,8 The most consistent deficits are in motor response inhibition, working memory, sustained attention, response variability and cognitive flexibility: in this regard, changes in temporal processing have been noted, especially with time discrimination and tasks that require time estimation.9
Adult ADHD is a common condition with multiple psychosocial consequences for the patient, so it is relevant to know the efficacy of adjunctive therapies to standard pharmacological treatment that impact on executive functions and cognition.10–13
The tDCS as an adjuvant in psychiatric conditions has evidence of usefulness in: depression, various meta-analyses support the use of anodic stimulation for the effective control of depressive symptoms. It has been shown to be useful in reducing cravings in randomised, double-blind trials in nicotine, marijuana and cocaine addicts. Encouraging results are also beginning to be published in relation to obsessive-compulsive disorder, eating disorders (bulimia - anorexia nervosa), tics, hallucinations in schizophrenia and dementias in which improvements have been noted in the working memory, spatial memory and word recall of those affected.5,14,15
The tDCS has also been used as an adjuvant in various neurological, neurodegenerative diseases (Parkinson’s), cerebrovascular disease in particular as part of neurorehabilitation for hemiparesis, aphasia, hemineglect and swallowing disorder.16
The aim of this work was to determine the effect of tDCS as an adjunct to standard treatment on cognitive attention function in adults with ADHD. Our research hypothesis was that the application of tDCS as an adjunct to standard treatment will improve performance on the d2 test by 20% in cognitive attention function compared to a control group.
2. Methods
Study design: Experimental, randomized, single-blind study in intervention and control groups; carried out in the cognitive rehabilitation unit of the Fray Bernardino Álvarez Psychiatric Hospital (FBAPH).
2.1. Sample size
The sample consisted of 43 participants, 23 in the intervention group and 20 in the control. The effect size of 1.6, alpha probability of 0.05 beta probability of 0.20 and standard deviation of response of 5 points. For the purposes of this study, a change of 20 points in the score on the d2 test will be considered as a positive response. Degrees of freedom = NT - 1 = 42, non-centrality parameter = δ = 2.87; E/S(Δ) = δ/√N = 0.45425; effect size E = E/S(Δ) x S(Δ) = 2.27.
2.2. Selection criteria for the intervention and control groups
Patients of both sexes, over 18 years of age, whose primary diagnosis was ADHD without other active Axis I diagnosis and treated with methylphenidate were included. Patients with a history of skull surgery, patients with intellectual disability of any degree, recent head trauma, history of primary or substance-related psychotic episodes, acute substance intoxication were excluded. Also excluded were patients with uncontrolled comorbid medical conditions, progressive brain disorders, epilepsy, severe systemic diseases, cardiac disease, chronic skin disease or damaged skin on the scalp, pregnancy or lactation; in addition, patients with cranial metal implants (except dental fillings and dental plates) or permanent medical devices (pacemaker, deep brain stimulator, drug infusion pump, cochlear implant, etc.). Patients who did not complete 100% of sessions were eliminated.
The main variables were gender, age, schooling, current ADHD treatment, ADHD profile, attention.
2.3. Procedure
Participants were recruited from the outpatient services of the FBAPH, invited to participate verbally, all questions were answered and informed consent was given. Those who chose to participate and signed the informed consent form were randomised. To randomise them, a system of red and black cards in sealed envelopes was used; participants chose an envelope containing a card. Those with red cards were integrated into the control group and those with black cards into the intervention group.
The Sooma TM tDCS stimulator was used to administer the stimulation.
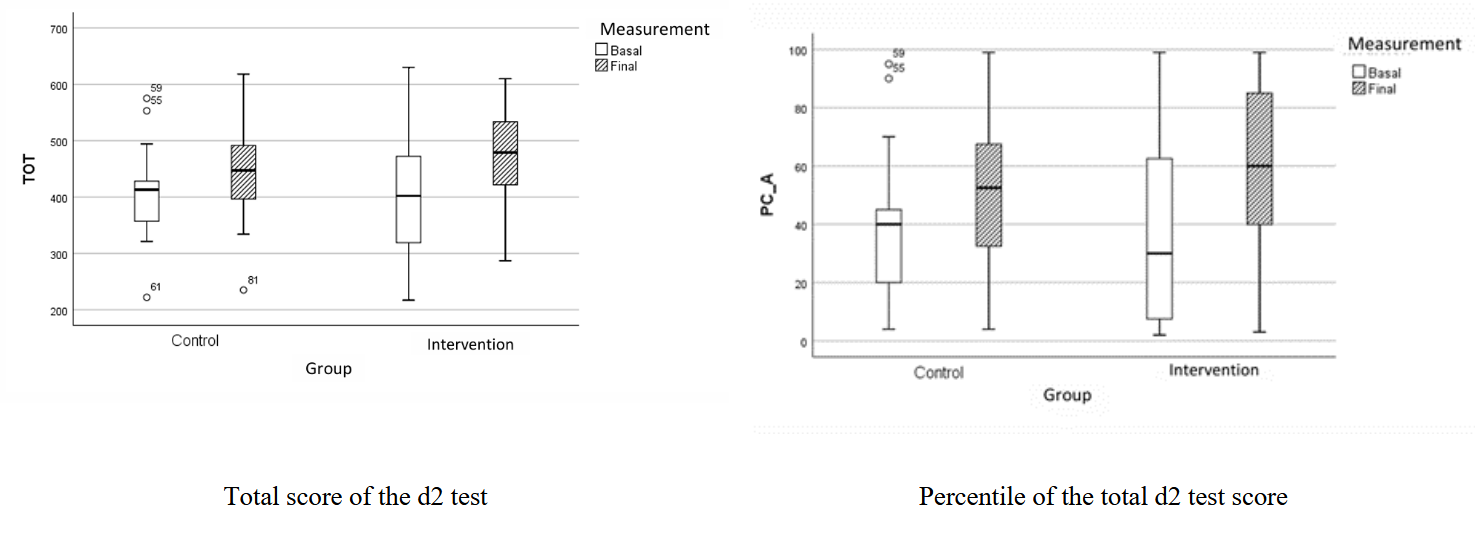
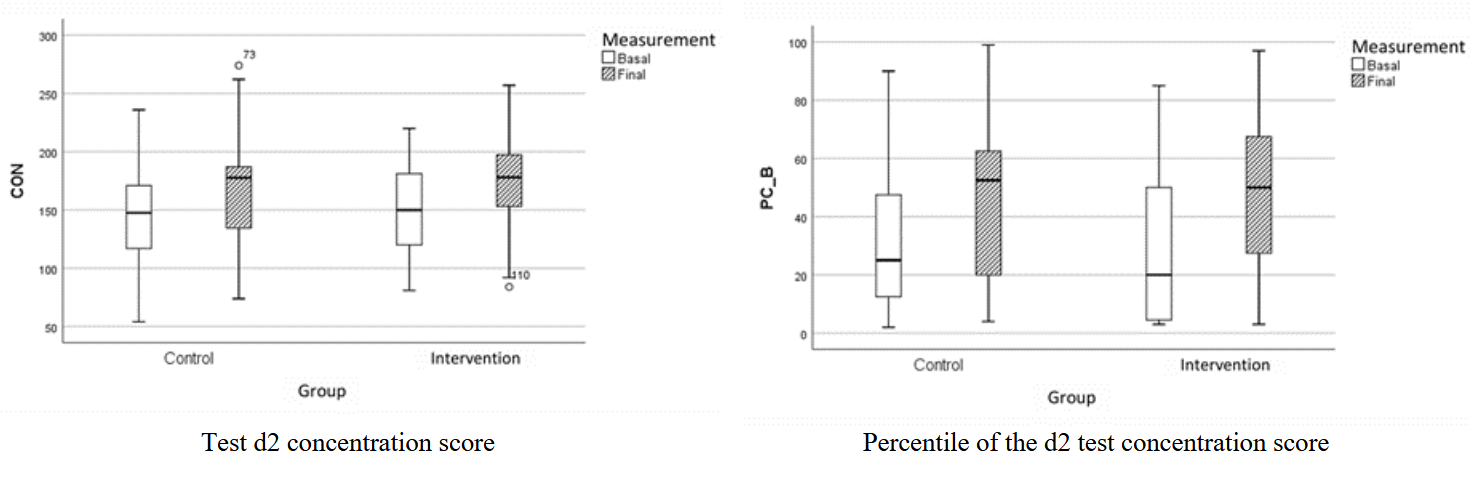
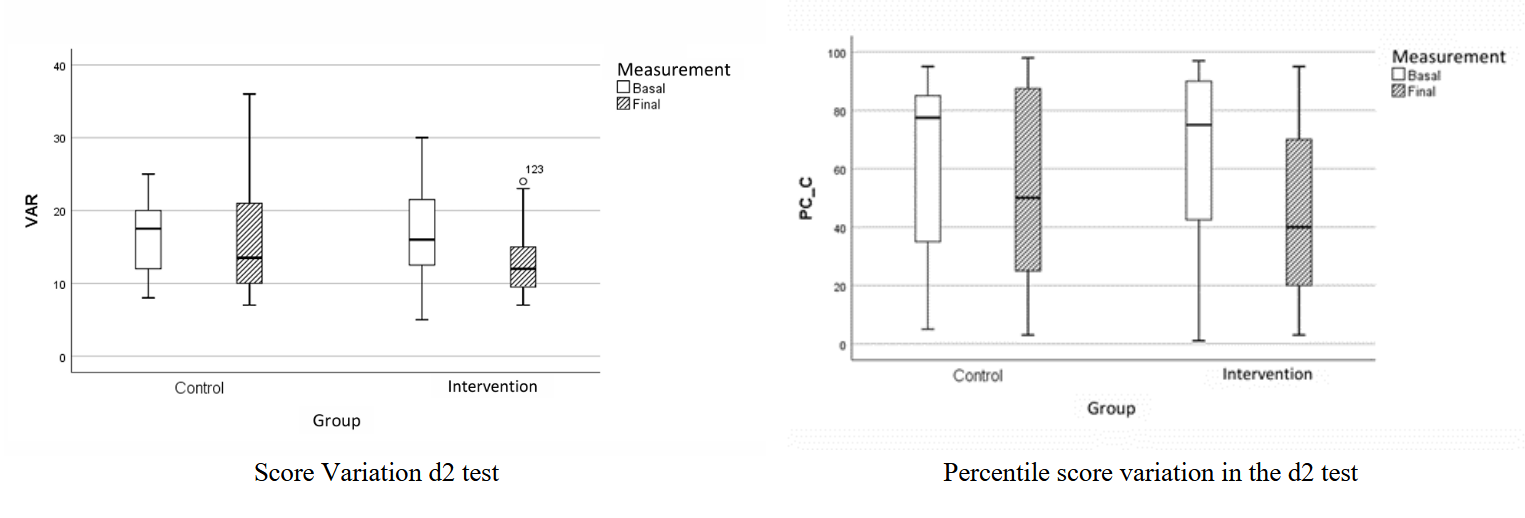
Prior to the first session and immediately after the conclusion of the total number of sessions, a test of attention Test D2 was administered, which consists of total score, concentration and variance. The total score (TOT) measures the total number of stimuli processed in the test and is a reliable measure of selective and sustained attention. The concentration variable (CON) reflects the number of relevant items correctly marked in the test, providing an index of the balance between speed and accuracy in the subjects’ performance. The variation variable (VAR) of the d2 test describes the difference between the highest and lowest productivity of the 14 lines of the test, assessing the consistency over time of the subject’s performance.17
To identify the clinical profile of ADHD of each study subject (inattentive, hyperactive-impulsive or mixed), the Adult ADHD Self Report Scale Symptom Checklist (ASRS) was applied.18
The electrode array used was bilateral in the dorsolateral prefrontal cortex region. The anodal stimulation was applied on the F3 position according to the international 10/20 system and the cathode was placed on the contralateral position (F4). A total of 15 tDCS sessions of 30 min duration and 2 mA intensity were applied to each participant in the intervention group. Participants in the control group were given 15 simulated sessions using the placebo mode of the equipment. Subjects in both groups attended daily to the rehabilitation service for 15 days for one session per day.
During and immediately after the application of tDCS, participants from both groups were asked to describe adverse effects with a questionnaire adapted from the proposed systematization of adverse effect reporting of tDCS.19
2.4. Statistical Analysis
For the description of qualitative variables, frequencies and proportions were used, while for the description of quantitative variables, the distribution of the data was first determined. The distribution of the data was verified with the Shapiro-Wilks test. Normally distributed variables were described with mean, standard deviation and median, interquartile and range were used for the description of freely distributed variables. To determine differences in proportions in qualitative variables, the Xi-squared test was used. In the case of qualitative variables, Student’s t-test was used to compare means for normally distributed variables, or the Mann Whitney U test when normality was not met. To determine differences in the intervention, Student’s t-test was used to compare baseline versus final means and standard deviation in each of the groups. The IBM® SPSS® version 25 statistical suite was used, and differences with a p<0.05 were considered statistically significant.
3. Ethical Considerations
The project was approved to the Research Committee registration 980 and Approved by Research Ethics Committees of the Psychiatric Hospital Fray Bernardino Álvarez (REC-PHFBA) on 24 June 2023. The REC-PHFBA is registered with the National Bioethics Commission under number 486. All participants signed informed consent.
4. Results
Forty-three patients with a diagnosis of attention deficit hyperactivity disorder were included, 23 (53%) of them were randomly integrated into the intervention group. No significant differences were found in age, sex, marital status or schooling of the two groups. Table 1
Regarding the clinical subtype of ADHD, the inattentive type was more frequent, with no significant differences between the groups. In terms of the ASRS v1.1 scale score, no statistically significant differences were found. Table 1.
Concerning treatment, the mean dose of methylphenidate was lower in the control group, but the statistical test showed no significant differences. Respect to adjuvant medication, the type of antidepressants was similar. The use of general medication is only described in terms of frequency. Table 1
The differentials between baseline and final scores were higher in the intervention group, with no statistically significant changes in the control group. In contrast, a statistically significant increase was found in the intervention group for total score (TOT) and for variance (negative) as expected. Table 2
As for the total score (TOT) a statistically significant change was obtained (t= -2.9, p<0.01), the location of TOT score obtained in the corresponding percentile, also resulted with significance (t=-2.8, p<0.01) corresponding to the end of the intervention, implying an improvement in the cognitive function of selective and sustained attention of the participants. Figure 1

The total CON score in the intervention group was close to being statistically significant (t= -2, p= 0.052), however, when the CON score is at the respective percentile, statistical significance was obtained (t= -2.4, p= 0.02), implying that the intervention subjects improved their ability to process stimuli correctly and accurately. The closeness to statistical significance of the CON score may be influenced by the sample size, with the possibility that, with a larger sample, a statistically significant result could be achieved. Figure 2

In terms of the variance variable (VAR), a statistically significant difference was obtained in the intervention group (t=2.3, p=0.02), and when the score was placed in the corresponding percentile, the result was close to being statistically significant (t= 2.0, p=0.051). It is considered that following the effective tDCS intervention, participants improved the consistency of their attention throughout the test performance. Figure 3

No statistically significant side effects reported by users were found in any of the groups. In the control group, headache 5%, mood disturbance 10%, itching 20% and drowsiness 10% were reported; for the intervention group, burning 9%, itching 35% and drowsiness 13% were reported. Table 3.
5. Discussion
The effect of tDCS as an adjunct to standard treatment on the cognitive function of attention in adults with ADHD was studied and we found that selective and sustained attention was 20% statistically significant, as was the consistency of attention in the test, while speed and concentration did not reach the expected 20%
These results coincide with those reported by Allenby,20 who documented a significant improvement in attention measured by the Continuous Performance Task test, with an improvement effect similar to that achieved with methylphenidate. Another study conducted in double-blind, placebo-controlled adults with diagnosed ADHD who received stimulation with anode in the right dorsolateral prefrontal region and cathode in the same region on the left side showed a decrease in symptoms assessed with the ASRS scale compared to the group that did not receive transcranial stimulation, with persistent improvement after the end of the sessions.21
In the current study, the anode was placed in the left dorsolateral prefrontal region, although several previous studies suggest that tDCS has an effect on attention or inhibitory control in this position.22 However, a randomized double-blind study in 60 adult ADHD patients using the go/no-go test before and after the sessions found a statistically significant difference between the control and experimental groups.23
Similar findings can be observed in children, a study conducted in children under 12 years of age with ADHD symptoms who underwent anodal tDCS on the right dorsolateral prefrontal cortex found that there was improvement in inhibitory symptoms, however, this is dependent on the severity of the symptoms.11 Another double-blind study in the same age group with a sample of eleven children undergoing cathodal tDCS on the left dorsolateral prefrontal cortex found improvement in inhibitory control but not in attention.24,25
Although tDCS has demonstrated a positive effect on cognitive and clinical functions in ADHD patients, these findings are encouraging but insufficient to support the use of tDCS as an alternative neurotherapy for ADHD, so it is important that future studies include larger samples that identify more optimal stimulation sites and parameters and that in combination with cognitive training could achieve more promising effects.26–28
6. Conclusion
The tDCS is useful for improving selective and sustained attention in adults with ADHD, with a positive effect on different components of executive function such as concentration and maintenance of effort over time with the anode in the left dorsolateral prefrontal position. It is also a safe therapy with mild and self-limiting side effects. Longitudinal follow-up studies are needed to determine the consistency of the effect over time and thus make treatment protocols more effective and efficient.
Funding
The project was developed in collaboration with Health for Better Neuroscience México who provided the Transcranial Direct Current Stimulation equipment and all supplies. Health for Better Neuroscience México did not participate in the structuring of the project and was not involved in the development of the project.
Disclaimers
The author’s statement that the views expressed in the submitted article are owns and not an official position of the institution or funder.