1. Introduction
Suicide is a leading cause of death among adolescents worldwide.1 Although in Latin America and the Caribbean, the suicide mortality rates are low (6.1 suicides per 100,000 inhabitants), in Mexico a steady increase is observed becoming the first cause of death in Mexico for adolescent women aged 10–19 years and the third cause of death among men. An analysis of trends between 1990 and 2017 reveals that the frequency of suicides has been on the rise (122.4% in adolescents from 10 to 14 years old and 81.4% in those of 15 to 19 years old).2 Globally, suicide ideation and attempts are strong predictors of suicide deaths with many individuals first ideating and attempting during their adolescent years.3 Thus, in Mexico, 6.5% of adolescents presented a lifetime suicide attempt in 2022.4
Suicidal behaviors emerge from the complex interplay of factors,5 including, but not limited to biological,6 psychiatric,7 psychological,8 and social risks.9 These risk factors influence each other in a dynamic manner over time.10 Most traditional research on suicidality fails to account for the dynamic interplay of risk and protective factors. As described by Franklin et al.11 in their meta-analysis of 50 years of research in suicide, most studies have rarely examined combined multiple risks in a “complex but replicable manner” (p. 32). Our limited understanding of the interplay of risks gravely impacts the effectiveness of prevention and treatment efforts in this area.
Prevention strategies are in need to rely on evidence documenting the following core facts: a) suicide rate in increasing in children,12 b) the rise in suicide and SB most likely affects those living in poverty or experiencing maltreatment12,13; c) effective intervention is to be developed where it occurs with the requirement to be responsive to the unique mental needs of the specific population studied14; d) the study of adverse events within a particular context is required in order to account for the specific social-individual level factors that shape suicidality in low-and middle-income countries (LMICs).15
It is essential to address the limitation of applying conventional suicide prevention models that are developed in high-resource settings and brought to low-income countries for implementation, neglecting the unique systemic, social, and individual-level factors.14 To this extent, only at the level of the role played by family factors in contributing to suicide, it is particularly important to point out that recent studies highlight how changing, dynamic and specific the structure and functioning of family in Mexico is.16 The understanding of its influence on the suicidal behavior of adolescents in Mexico can only be understood from a) the diversification of its structures, b) the displacement of authoritarian modes towards interactive modes, and c) the coexistence of elements of modernity with traditional ways.16
Simultaneously, there is increasing attention to the potential of data sciences to improve suicide risk research.17 This is because data sciences methods, such as machine learning (ML), are suited to explore high-dimensional interactions of risk. Burke et al.18 identified three main contributions of ML in suicide research: ML can improve the accuracy of risk prediction, identify important risks and define their interactions, and model risks across subgroups of individuals. More scientists are applying data sciences to study the suicidal behaviors of adolescents19 and adults.20
Although adolescent suicidality has been widely studied in high-income countries, there is a significant lack of evidence from low- and middle-income countries (LMICs), particularly regarding clinical populations receiving psychiatric care. In Mexico, little is known about the combined impact of psychiatric disorders and adverse life events (ALEs) on suicidality among low-income adolescents. Existing studies often examine these factors separately, overlooking their complex and potentially interactive effects. Moreover, prevention models developed in high-resource settings may not adequately reflect the cultural, social, and systemic realities influencing suicidality in Mexican youth. The application of machine learning (ML) to this problem has not yet been explored in this context, despite its capacity to capture high-dimensional interactions between risk factors. We hypothesize that suicidality in low-income Mexican adolescents receiving psychiatric care is best explained by an interplay between psychiatric disorders—particularly affective disorders—and ALEs, especially those involving family dysfunction, social adversity, and experiences of abuse.
This study aimed to analyze the impact of psychiatric disorders and adverse life events on suicidality in a clinical sample of low-income adolescents from Mexico’s main child psychiatric hospital.
2. Method
2.1. Study design and participants
This cross-sectional predictive study used a non-probabilistic clinical sample of 127 adolescents (66% female) aged 10 to 17 years (M = 14.4; SD = 1.6), selected from a larger group receiving mental health services at the Juan N. Navarro Children’s Psychiatric Hospital. This hospital primarily serves children and adolescents from low socioeconomic backgrounds (Table 1). Most participants lack health insurance21 and come from suburban areas of Mexico City, which are characterized by low social development, high poverty levels, and significant marginalization.22
2.2. Variables and measures
Psychiatric disorder. The Mini International Neuropsychiatric Interview for Children and Adolescents23 was used to assess the number and type of psychiatric disorders. The assessment covered 17 Axis I diagnoses from the DSM-IV and ICD-10 categorized into affective, anxiety, substances, conduct, and eating disorders.
Adverse life events. We focused in the presence/absence of negative life events that increase an individual’s emotional vulnerability that is perceived as threats. The Questionnaire of Life Events for Adolescents (QLEA),24 is a self-report that evaluates 128 positive and negative life events in seven domains. For this study, 81 negative life events items from six domains were extracted (Failure 5, Family 37, Health 10, Personal 15, School 5, and Social 10). Due to the exclusion of items with low prevalence, only 59 final items were included in multivariate analyses. The QLEA has shown good psychometric properties such as temporal stability (r = 0.75) and convergent validity with similar measures (r = 0.76). Recent psychometric evaluations support its continued use in Latin America.25
Suicidality. Suicidality is broadly defined as a spectrum of wishes, ideas, and behaviors, ranging from suicidal ideas, suicidal plans, and suicide attempts implying any deliberate action resulting or not in death.26 We used a Mexico/Spanish 6.0 version of the Suicidality Module of the Mini Kid International Neuropsychiatric Interview for Children and Adolescents.23 Section B “Suicidal Behavior, self-injuries, and suicidal ideation” consisting of 13 dichotomous items was used, providing suicidality indicators that assess during the last month suicidal wishes (Did you feel so bad that you wanted to end your life?); suicidal ideation (Did you think of harming or hurting yourself or Did you have mental images of harming yourself with at least some slight intent to die?); self-injuries (Did you try to hurt yourself in an accident, either actively or passively?); suicidal plan (Did you have any plans to take your life?); suicidal attempt (Did you try to kill yourself?). Some psychometric properties are well documented (e.g., inter-rater reliability: kappa coefficient = 0.95).27
Socioeconomic Status (SES). The SES was assessed based on parental education and occupation. Conducted by social workers, the Socioeconomic Evaluation Study (SEE) evaluates income (55%), occupation (10%), expenses (10%), housing (20%), and health (5%). Patients are classified into SES levels (low to high), to prioritize resources and guide social interventions. Its validity and reliability in Mexican health institutions are documented.28
2.3. Procedure
The participants were adolescent inpatients recruited from the hospitalization service, who underwent a comprehensive assessment using several instruments, including the Socioeconomic Evaluation Study (SEE), the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID), and the Questionnaire of Life Events for Adolescents (QLEA). Based on SEE and MINI-KID data, adolescents with a socioeconomic status above the lower-middle level and those diagnosed with psychotic disorders were excluded from the sample. The final sample consisted of 127 adolescents, classified according to the presence or absence of suicidality. Their data were included in the analyses.
All instruments were administered by trained psychiatrists and psychologists from the research team, who also provided clarification as needed. Informed assent and consent were obtained from the adolescents and their parents, respectively, after explaining the study’s objectives. The research protocol was approved by the Institutional Research and Ethics Committees of the Child Psychiatric Hospital (registry number II3/01/0412).
2.4. Statistical analyses
Because under the ML approach there is no practical guideline to evaluate the sample size,29 we carefully followed the strategies suggested by Vabalas.30 That is, in order to obtain robust and unbiased estimates regardless the sample size, the original sample was randomly split in train/test and using nested cross validation key parameters were tuned.30 Since the applied classification algorithms do not assume a normal distribution we did not performed normality test.
The presence of suicidality was established from a positive response to at least one of the 13 items. This dichotomous suicidality item was used as the primary outcome variable. Group differences were tested with Pearson’s χ² test for categorical variables and Welch’s t test for the continuous variables. In order to identify key predictors, continuous variables were first standardized and then using a machine learning approach, classification algorithms including classification tree (CT), random forest (RF), XG-Boost (XGB), and logistic regression (LR) were performed. The area under the ROC curve (AUC) was used as the main measure of the predictive performance of all models. Aiming to improve interpretability, the importance of each variable on the accuracy of each predictive model was also quantified. Accepted statistical significance was P<=0.05. Analyses were conducted with RStudio under R version 4.4.3.31
3. Results
More than half of the participants presented suicidality. We observed significant differences between participants with suicidality and without suicidality in the prevalence of affective pooled diagnoses and eating diagnoses. Differences between these groups were also detected in the prevalence of specific categorical diagnoses such as the presence of depressive disorder and dysthymia, separation anxiety disorder, social phobia, generalized anxiety disorder, and post-traumatic stress disorder. No statistically significant differences were found in the rest of the diagnostic categories. Regarding ALEs the differences observed were as follows: a) in the family domain of the twenty-five items assessed only four showed differences between the participants with suicidality and without suicidality; b) in the social domain the differences observed were for four items out of nine; c) in the personal domain, differences were observed in only one of the eight items, although it was not statistically significant; d) in the health domain the difference was observed only in one item out of ten; e) in the school domain the difference observed was also for one item out of four; finally, f) in the failure domain no item showed significant differences (Table 2).
Machine learning: prediction models and performance measures. Table 3 shows the predictive performance of the four models through the estimation of six parameters. In comparing the point estimates of AUC, RF showed the best diagnostic performance, followed by CT and LR. XGBoost had the lowest performance, however, the 95% confidence intervals for all of them overlapped. In terms of accuracy, sensitivity, and specificity, the models obtained by RF and XGBoost have the best balance between parameters, CT had high sensitivity but at the expense of specificity, and the model by LR possessed the lowest values for all of these. According to the widely cited guideline suggesting that the positive and negative likelihood ratios of 2 to 5 and 0.5 to 0.2 (respectively) generate small, but sometimes significant changes between pretest and post-test probabilities,32 CT, RF, and XG Boost fall into this category; the LR-derived model can be considered to be less useful as a diagnostic test than these. Nevertheless, these parameter estimates also overlapped when looking at their 95% confidence intervals, and no conclusions could be drawn as to the superiority or inferiority among the models. One thing that can be pointed out is that the confidence intervals for the positive and negative likelihood ratios for the LR include 1, which implies the possibility of no effect on the post-test probability, whereas, for the other three models, it is undeniable that a positive or negative result would change the post-test probability, even slightly.
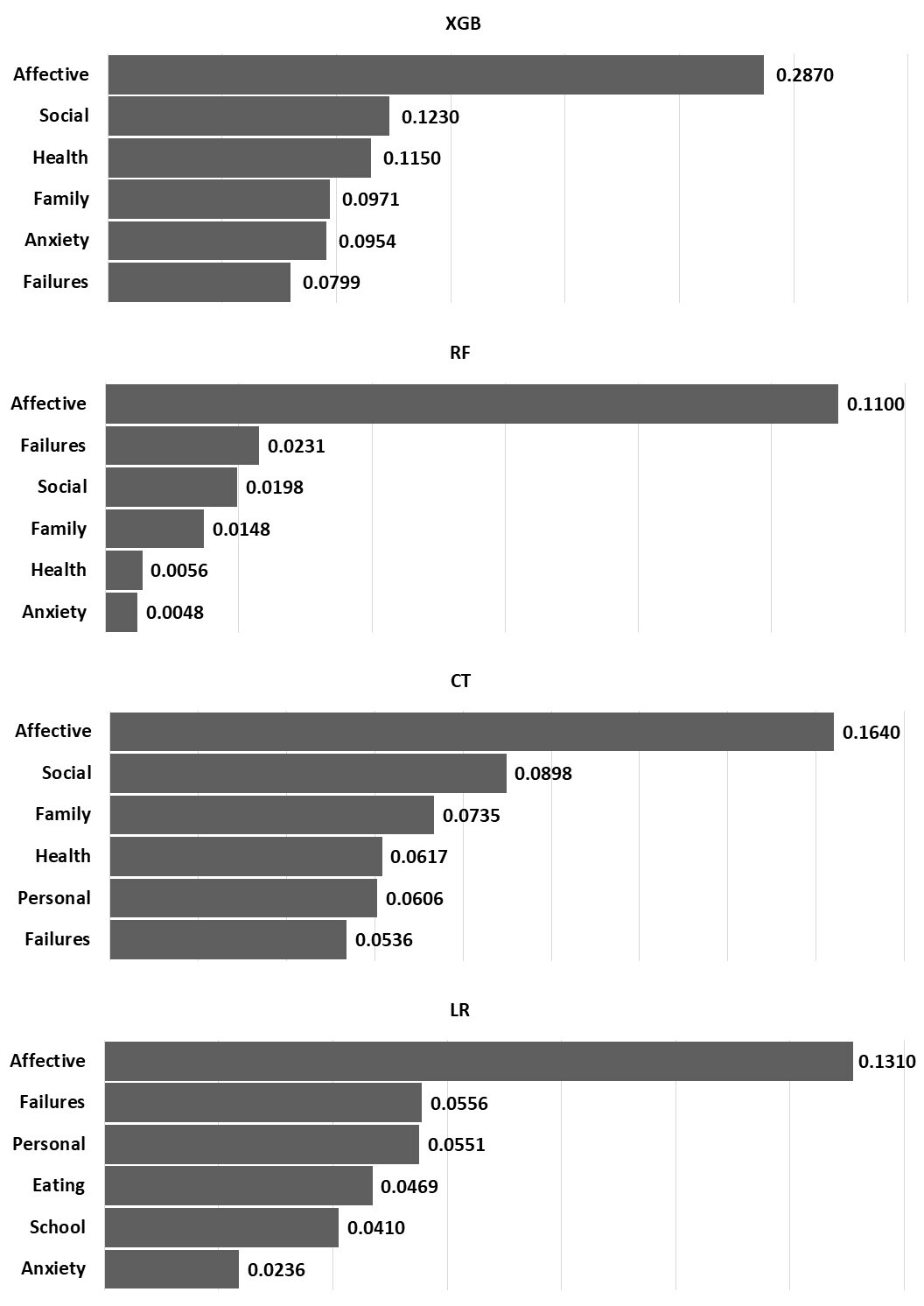
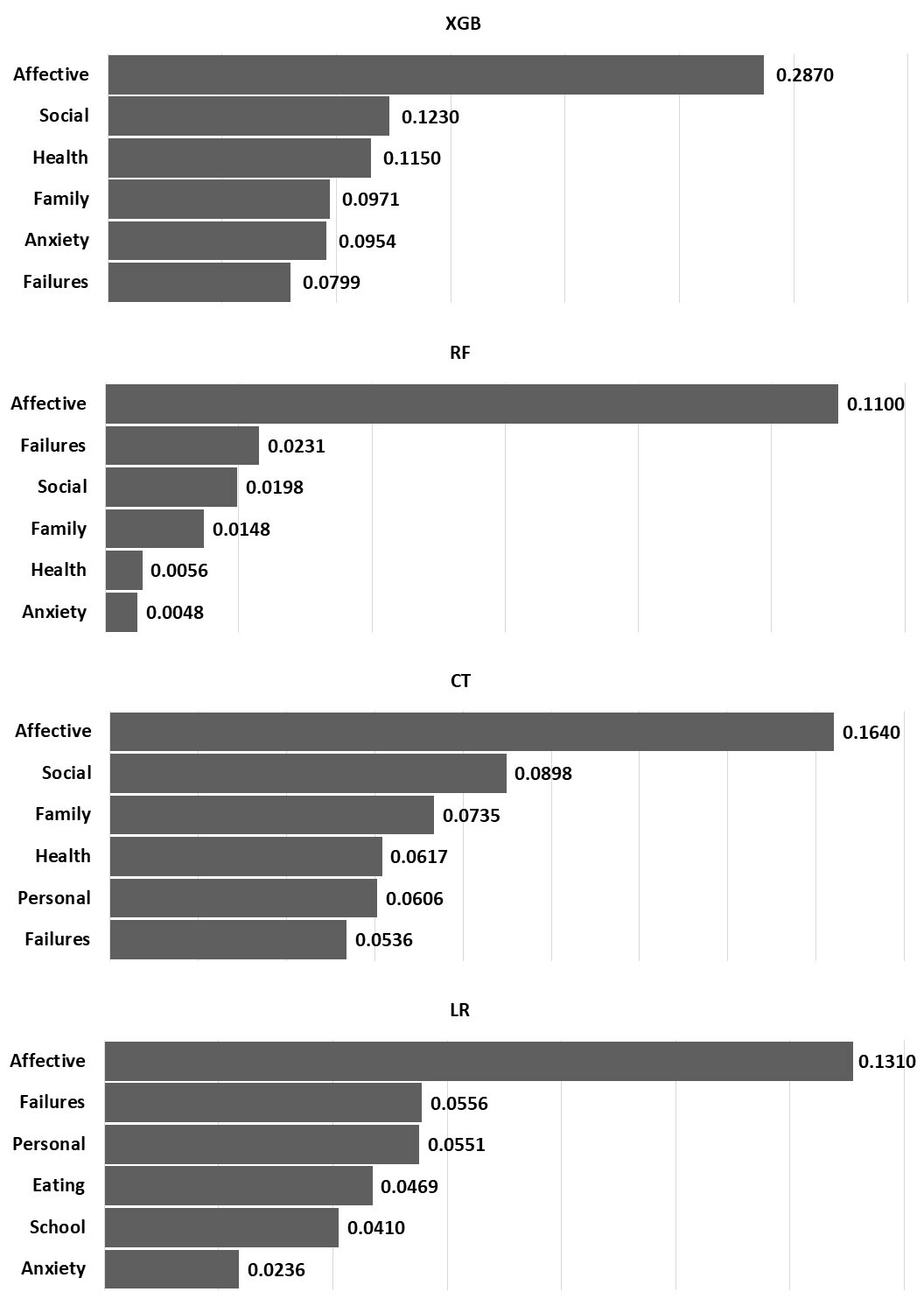
In all four prediction models, the most important predictor was affective disorder. Family, health, failures, and social adverse life events appeared as the most important even ahead of other psychiatric disorders. Anxiety disorder was also relevant in all models, followed by conduct disorders, and to lesser degree eating disorders, emerged as a predictive variable in LR model (Figure 1).
The results across the four predictive models (XGB, RF, CT, and LR) consistently highlight affective disorders as the most important factor associated with suicidality in adolescents. In all models, affective symptoms demonstrated the highest importance score, with particularly strong influence observed in the XGBoost model, where it nearly tripled the weight of the next most relevant variable.
Beyond affective symptoms, social and family-related life events also showed considerable predictive value, especially in the XGBoost and CT models. These results suggest that difficulties in interpersonal relationships and family dynamics may significantly contribute to suicidal behavior. Health-related issues and anxiety symptoms appeared as moderately relevant predictors, though their importance was more pronounced in the XGBoost model and substantially lower in RF and LR.
Failures and personal life events were particularly relevant in the LR and CT models, indicating that adolescents’ responses to difficulties and personal challenges may also play a role in suicidal risk. Interestingly, eating and school-related life events were unique to the LR model, where they carried modest but notable importance.
Overall, the findings underline the central role of affective disorders in adolescent suicidality, while also pointing to the importance of social and environmental stressors, particularly those related to family, social contexts, and personal failures. The variability in predictor importance across models highlights the value of using multiple analytic approaches to capture the complexity of factors contributing to suicidal behavior.
4. Discussion
The study’s findings support our hypothesis that suicidality in low-income Mexican adolescents receiving psychiatric care is best explained by the interplay between psychiatric disorders—particularly affective disorders—and adverse life events, mainly family dysfunction, social adversity and experiences of abuse. To our knowledge, this is the first study to apply ML in a clinical low- and middle-income country (LMIC) setting to assess suicidality among adolescents. Our approach aligns with recent calls to identify context-specific risk factors that inform mental health strategies tailored to adolescents in LMICs.33
We implemented four ML models (Classification Tree, Random Forest, XGBoost, and Logistic Regression) and evaluated both their predictive performance and agreement. These models consistently identified affective disorders as the strongest predictor of suicidality, confirming previous evidence from high-income countries (HICs).10,34 Importantly, our models demonstrated fair predictive accuracy and good calibration, suggesting they reliably estimate suicidality risk and could guide resource allocation in under-resourced clinical settings.
The prevalence of suicidality in our sample was notably higher than that reported among Hispanic adolescents in other tertiary care settings.35 This likely reflects the limited availability of community-based services in Mexico, meaning that only the most severe cases reach specialized care. Consistent with prior studies in Latin America36 and in USA psychiatric populations,37 affective disorders were highly prevalent (76%) and significantly more frequent among suicidal adolescents (90%) compared to non-suicidal ones (57%). Anxiety disorders were also prevalent (52%), with their association to suicidality aligning with longitudinal findings from Mexico,38 global data from LMICs39 and HIC37 particularly in terms of maintaining suicidal behavior over time.
Eating disorders also emerged as relevant risk factors, corroborating findings from studies in HICs.40 Beyond psychiatric diagnoses, our study highlights the importance of ALEs in suicidality risk. Despite increasing attention in the global north, these factors remain underexplored in many LMICs, including Spain.41 In our sample, family-related adversities such as physical abuse and changing household dynamics (e.g., mothers entering the workforce) were significant contributors to suicidality. These results align with prior findings on youth in Mexico42 and other LMICs.43,44 stressing the urgency of addressing psychosocial adversity in prevention efforts.
Moreover, our findings emphasize the alarming prevalence and impact of sexual violence. One in four suicidal adolescents reported experiencing sexual abuse or rape, nearly double the rate found among their non-suicidal peers. These rates far exceed those observed in community-based samples in Mexico,42 and align with recent national data showing that sexual abuse is strongly associated with a range of negative outcomes, especially suicidal behavior.45 These results underline the urgent need for targeted interventions addressing sexual violence as part of comprehensive suicide prevention efforts in Mexico.
Equally important, this study emphasizes the role of peer relationships in adolescent suicidality. Consistent with previous findings,43,46,47 lacking friends, losing peer connections, or experiencing deteriorations in friendship quality significantly increased suicide risk. These social dimensions are often overlooked in clinical assessments, yet they represent vital targets for preventive interventions.
Lastly, high body weight also emerged as a differentiating factor, with findings supporting prior research on the impact of weight-based stigma on adolescent mental health and suicidality.48 Together, these results advocate for integrated, multidimensional prevention strategies that address psychiatric disorders, social adversity, and broader structural vulnerabilities affecting adolescents in LMICs.
Machine learning models demonstrated fair predictive accuracy and could be useful for guiding resource allocation in under-resourced clinical settings, though model improvements are needed.
5. Limitations
This study has several limitations that should be considered. First, the cross-sectional design precludes causal inference, limiting conclusions to associations rather than directionality of effects. Second, our relatively small and non-probabilistic clinical sample from a single national psychiatric hospital may reduce generalizability to broader populations, including community or outpatient samples. Third, reliance on self-report measures for adverse life events could introduce recall bias, particularly in emotionally charged experiences. Fourth, although multiple machine learning models were evaluated, the moderate performance and overlapping confidence intervals suggest that predictive accuracy could be improved with larger samples and incorporation of biological or psychosocial biomarkers. Finally, the exclusion of psychotic disorders restricts applicability to this subgroup of adolescents at risk.
6. Conclusions
Our findings underscore the central role of affective disorders in adolescent suicidality within this low-income Mexican clinical sample, consistent with patterns observed in high-income countries. Additionally, adverse life events—especially those related to family dysfunction, social adversity, and personal trauma—emerged as important contributors to suicide risk. These results highlight the need for culturally sensitive, multidimensional prevention and intervention strategies that address both psychiatric symptoms and psychosocial stressors. Future research should use larger, longitudinal samples to improve predictive modeling and explore mechanisms underlying these complex interactions.
Ethics statement
Informed consent was obtained from all participants included in the study. All procedures in studies involving human participants were performed in accordance with the ethical standards of the institution’s Human Research Ethics Committee. Ethical approval number: II3/01/0412.
Data availability
The authors will provide the raw data underlying the conclusions of this article upon request, without unnecessary restrictions.
Funding
This work did not receive any funding.
Authorship contributions
All authors contributed to the conception and design of the study. MEMC and BBE wrote the first draft of the manuscript. Material preparation and data collection were conducted by VPB, while data analysis was performed by CM and HMM. All authors provided feedback on earlier versions of the manuscript and approved the final version.
Disclosure of interest
We declare no conflict of interest.
Acknowledgements
The authors acknowledge the institutional support provided by the Child Psychiatric Hospital ‘Dr. Juan N. Navarro’ and the PAPIIT (research project IT300223) from the National Autonomous University of Mexico, which facilitated the execution of this study.
Corresponding authors:
1. Blanca Estela Barcelata Eguiarte.
Department of Psychology, Faculty of High Studies-Zaragoza, National Autonomous University of Mexico. Av. Guelatao 66, Ejército de Oriente Indeco II Issste, Iztapalapa, 09230 Ciudad de México, México. Email: bareg7@hotmail.com
2. Maria Elena Marquez-Caraveo.
Hospital Psiquiatrico Infantil “Dr. Juan N. Navarro”, CONASAMA, Secretaria de Salud, San Buenaventura 86, Colonia Belisario Dominguez, Alcaldia Tlalpan, CP 14080, Ciudad de Mexico, Mexico. Email: malenamarquezc@gmail.com