.tif)
1. Introduction
Mental disorders were the second leading cause of disease burden in terms of years lived with disability (YLDs) and the seventh leading cause of disability-adjusted life-years (DALYs) globally in 2019.1
Among those affected, mental disorders contribute to increased disability, morbidity and mortality and have adverse social and economic consequences. The burden of illness seriously impact health systems, particularly in low resource settings such as low- and middle-income countries (LMICs).2,3 Notwithstanding, evidence shows a deficit policy and program response to the mental health needs of populations in LMICs.3–7
India comprises around 18% of the global population and significantly contributes to the global burden of mental disorders. In 2019, mental disorders were the second leading cause of YLDs, and self-harm and violence were the tenth leading cause of death.1 Evidence suggests suicide deaths increased by 40% from 1990 to 2016 making it the third leading cause of death in several Indian states.2
India was one of the first few LMICs to develop a National Mental Health Programme (NMHP) addressing the mental health needs of the population. This paper discusses the history of India’s mental health response and reviews the NMHP to suggest the way forward. It aims to answer the following research question: How has India responded to the mental health needs of its population through the National Mental Health Programme in the last decade?
2. Methods
Review of literature was conducted on PubMed and Medline using the search terms “National Mental Health Programme AND India” and “District Mental Health Programme AND India”. Relevant documents on NMHP and District Mental Health Programme (DMHP) from the Ministry of Health and Family Welfare (MoHFW), Directorate General of Health Services (DGHS), Common Review Mission (CRM) (2012 to 2019), NITI Aayog and National Institute of Mental Health & Neurosciences (NIMHANS) were also analyzed. The duration was restricted to the past nine years from 2012 to 2021 to obtain the recent developments on NMHP since the 12th Five Year Plan. For that, articles that informed NMHP before the 12th Five Year Plan were excluded during the literature search (n=31). Based on the eligibility criteria, a total of 29 studies were included. A search strategy using PRISMA can be reviewed in Appendix 1. This paper follows a narrative style.
3. Setting the scene
This section illustrates the history of India’s mental health initiatives since 1946 to 2020 depicted in Fig. 1
.tif)
3.1. Initiatives prior to the establishment of NMHP
The Bhore committee report (1946) illuminated the status of mental health in India before independence. The report recommended a plan for increasing hospital beds and number of mental health institutions at the Center and DGHS level in country, training human resources and dedicating a mental health department in the proposed All India Institute of Mental Health.8
The Mudaliar Committee report (1962) recommended operationalizing in-patient and outpatient departments in hospitals, establishing specialized psychiatric mental health clinics/institutions and developing psychiatric clinics with a capacity of 5-6 beds in each district. The Srivastava Committee 1974 recommended the Community health volunteer (CHV) scheme focusing on identification and management of mental health disorders.9
A WHO expert committee meeting on “organization of mental health services in developing countries” held in 1974, at Addis Ababa expressed serious concern over burden of mental disorders and a significant treatment gap and asserted mental health care in developing countries.10 WHO Mental Health Advisory Group (1979) initiated a formal resolution urging member countries to develop NMHP to provide mandatory mental health care through the existing healthcare system.11 India was the first major country to launch the National Mental Health Programme (NMHP) in 1982.
3.2. Inception of NMHP
The GOI launched the NMHP in 1982, in response to the heavy burden of mental illness and critical need of mental health care infrastructure in the community. NMHP was re-strategized in 2003 to include modernization of state mental hospitals, and upgradation of psychiatric wings of medical colleges/general hospitals. Subsequently, the Manpower development scheme was added to NMHP in 2009. The three main components of the NMHP include prevention and promotion, treatment, and rehabilitation of mental disorders.12 The specific objectives of NMHP are to ensure the availability and accessibility of minimum mental healthcare for all in the foreseeable future; encourage the application of mental health knowledge in general healthcare and in social development; promote community participation in mental health service development; and enhance human resources in mental health sub-specialties.12
Strategies to achieve these objectives include integration of mental health services with primary health care through the NMHP; provision of tertiary care institutions for treatment of mental disorders; and eradicating stigmatization of mentally ill patients and protecting their rights through regulatory institutions like the Central Mental Health Authority (CMHA), and State Mental Health Authority (SMHA).12
3.3. Inception of DMHP
A pilot study (1985-1990) conducted in the Karnataka to assess the feasibility of districts to deliver mental health services demonstrated significant success and the potential for scale-up. Following which, the DMHP was appended to the NMHP in 1996 to overcome the shortcomings of the programme and transitioned the districts into administrative and implementation units for NMHP.11 The DMHP envisages extending mental health services through the existing healthcare infrastructure and human resources at the community level.11
.png)
DMHP has an objective to provide sustainable basic mental health services to the community and integrate them with existing health services; early detection and treatment of patients within the community; to reduce the stigma of mental illness through public awareness; and to treat and rehabilitate patients within the community.11
3.4. Policy prescription and legal probabilities
The National Mental Health Policy, 2014 aims to promote mental health, prevent mental illness, enable recovery from mental illness, promote de-stigmatization and de-segregation, and ensure socio-economic inclusion of persons with mental illness (PWMI) by providing accessible, affordable, and quality health and social care to all persons through their lifespan within a rights-based framework.13
The Mental Healthcare Act (MHA) passed in 2017 revoked the Mental Healthcare Act, 1987 which was under scrutiny for not recognizing the rights of PWMI. In addition to recognizing the rights of a PWMI, and thereby facilitating access to care, the act repealed Section 309 of the Indian Penal Code which criminalized attempt to suicide by PWMI.14
Additionally, the CMHA, SMHA and Mental Health Review Boards for regulation and co-ordination of mental health services under the central and state government was constituted. While there may be a silver lining to its development, it comes with the necessity of capacity building for effective implementation. CMHA and SMHA have not been instituted in many states.14
In the NHP 2017, mental health policy has been recognized as one of the policy-thrust areas.15
3.5. Vertical to complete integration
In 2018, GOI announced that Health and Wellness Centers (HWCs) would be created by transforming existing primary level healthcare facilities to deliver Comprehensive Primary Healthcare (CPHC) to achieve Universal Health Coverage. Under CPHC, Operational Guidelines for Mental, Neurological and Substance use (MNS) disorders care were launched in December 2020 with an objective to integrate mental health care services at HWCs.16,17
4. Experiences so far
The section will review NMHP’s progress, achievements and challenges by reviewing available literature between 12th Five Year Plan (2012) and 2021.
4.1. Issues concerning the development process of NMHP
The launch of NMHP received lukewarm support from the psychiatry community due to its problematic structure.4 With the gradual progression of the programme, several gaps in human resources (HR), transparency surrounding the responsibilities of health care professionals, managerial skills at the community level,5 funding,6 and a well-established monitoring and evaluation system7 were established.
The advancement of DMHP was influenced by the lack of mental health outreach services in other districts.18 The model was deficient being focused on pharmacological interventions and not including the psychosocial aspects of treatment.18 It excluded community/stakeholder participation in the planning and implementation process that further attributed to its poor performance.18 Currently, it’s implementation at the sub-district level and below is sub-optimal.18
4.2. Administrative issues
Fragmented responsibilities across levels and departments and poor coordination contributed towards the poor performance of the programme.7 The situation mandated the employment of a designated structure with sufficient funds and HR in the form of implementation teams at the central and state level that led to the constitution of CMHA and SMHA as advised by the Mental Health Care Act 2017.7
Nevertheless, the 13th CRM conducted in 2019 reported the constitution of SMHAs in addition to district level review boards in Chhattisgarh and Jharkhand.19 The role of Nodal Officers towards the successful implementation of the programme has been documented in several studies. However, lack in leadership and enthusiasm across levels further impacted program implementation.20
4.3. Financial issues
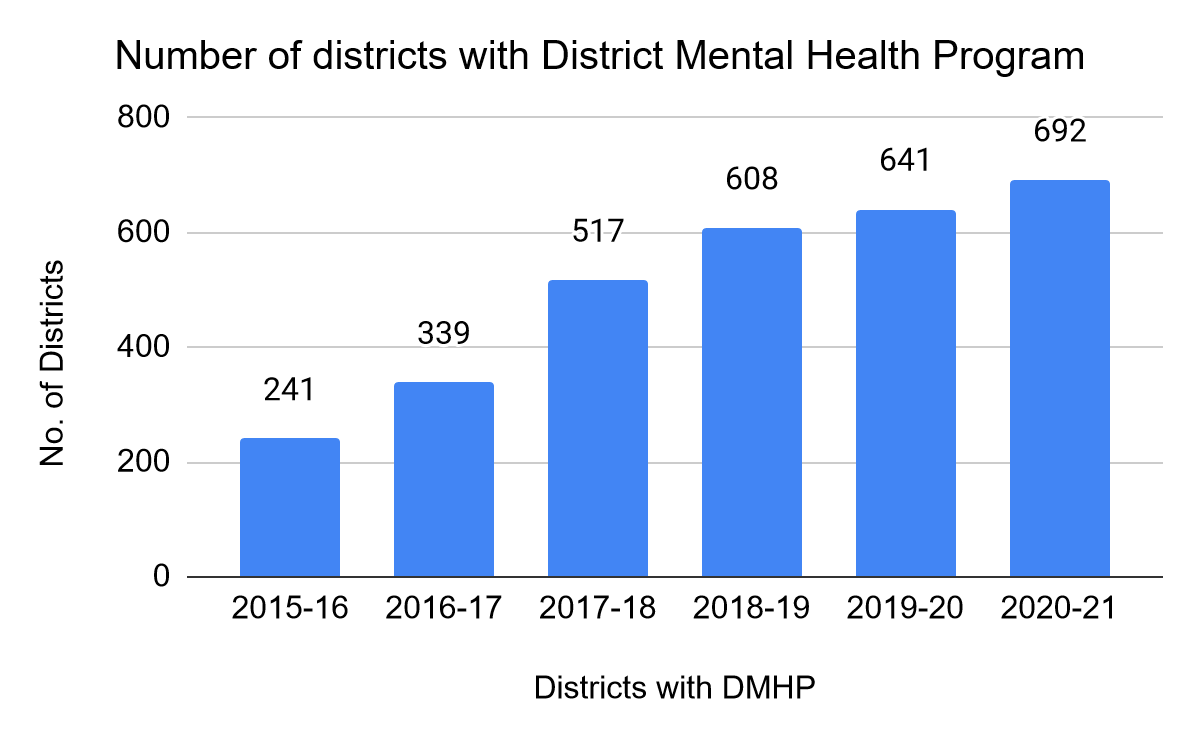
A major theme that emerged from the reviewed literature is the shortage of funds. The budget allocated to the NMHP was reduced from Rs 50 crore in Financial Year 2018 (FY18) to Rs 40 crore in FY1921 without explanation. Although the total healthcare budget was increased by 7 percent in FY20 and a substantial 137% in FY21, funding for NMHP remained the same at Rs 40 crores.21 Out of the total Rs 597 crore mental health budget in FY21, a major proportion of budget was allocated for State level institutes of Mental Health in Karnataka and Assam.21 Financial support available per DMHP is Rs. 83.2 lakhs and a total of 692 districts exist as of 2020-21.21 This huge shortfall of funds may eventually manifest an increase in burden of mental health illness with long-term implications on the country’s economy.
The estimated budget for the successful implementation for MHA, 2017 is around Rs 94,073 crore; however, expenditure during FY18 and FY19 is approximately Rs 5 crores for each year for NMHP, which signals gross underutilization of funds.22 A recently published evaluation report on the centrally sponsored schemes in India reported that the utilization of funds reduced to 0% in 2019-20 from over 100% in 2017-18.23
The funding for NMHP is split between the Centre and states in the proportion of 60:40, and 90:10 for special category states.24 Although states take financial responsibility of the program, implementation is incoherent due to pre-existing financial constraints within states.24
4.4. Issues related to human resources
The shortage of HR has been an issue since the inception of the NMHP. Lack of leadership at different stages of the hierarchy in addition to poorly skilled and remunerated health professionals have further attributed to the underperformance of the programme. The CRM reports have frequently highlighted the need for overstretched system to accommodate the additional burden of mental health diseases.25,26
With government augmenting the HR availability to deliver mental healthcare services, 0.29 psychiatrists per 100,000 existed in India in 2017.27 Developed nations have reported 6 psychiatrists per 100,000 population, which denotes India lagging substantially in HR for mental health compared to high-income countries.27 The availability of psychiatrists varies from 0.5 in Madhya Pradesh to 1.2 per 100,000 population in Kerala.27 Maharashtra stands out in organizing a mental health clinic at selected district with a psychiatrist, a psychiatric social worker, and an occupational therapist and staff nurse20 The current status of HR can be reviewed in Table 1.
Previously, the training provided under DMHP was lacking in terms of duration, specialist support and refresher courses, and was predominantly biomedical and failed to incorporate the psychosocial aspects.18 To overcome those challenges, the Indian government established a Digital Academy in NIMHANS Bangalore, CIP Ranchi and LGBRIMH Assam for large scale digital training of medical doctors/officers, psychologists, social workers and nurses in mental health.23 Details can be reviewed in Table 2.
4.5. Monitoring and evaluation issues
Standard formats for recording and reporting have been developed for monitoring and evaluation purposes. Additionally, a central mental health information system (MHIMS) has been positioned with a budget of 40 million INR with clearly defined indicators, data sources, and reporting protocol and linked to a national surveillance system.28 The MHIMS facilitates bilateral communication between participating units with the potential to improve implementation through mid-course correction based on the feedback.28 Nevertheless, evaluation of the activities under NMHP is yet to be conducted periodically.4
4.6. Public–Private Partnership
Initially, the DMHP primarily relied on the public health facilities for service delivery without private sector involvement. However, public health facilities being resource constraint, could provide services to a limited population.18 This impacted DMHP’s scale up and implementation which further affected the success of NMHP.
Addressing the challenges, GOI introduced the Public–Private Partnership (PPP) Model component under NMHP. Under this, provisions have been made for the state governments to execute activities related with mental health in partnership with Non-Government Organizations (NGOs)/Agencies as per the NHM guidelines.28 The government invites and supports the private sector by providing financial aid to provide community care through Day Care Centre, Residential/Long-Term Continuing Care Centre and Community Health Center.28
4.7. Community participation and IEC activities related issues
Studies demonstrated that DMHP was adversely impacted due to lack of awareness and stigma in many states.4 A lack of comprehensive evidence-based IEC/BCC plan was also established. Where available, the planning of IEC/BCC strategies were done at the state level with minimal districts involvement, and were more of programme related awareness.25 IEC/BCC monitoring was observed as an area of concern across states.25 This is adjunct by HR shortfall for IEC , lack of locally relevant and conceptualized IEC materials with focus on the physical presence of IEC materials than on enabling their utility for awareness among beneficiaries.25
Addressing this, GOI recently allotted 450 million INR for IEC activities in the form of launching websites and TV/radio programs to promote mental health awareness.23 Furthermore, the CIT and SITs are established to ensure effective community participation through Mental Health Care Committees (MHCCs), caregiver groups, user groups and Jan-Sansad.4
4.8. Coverage and provision of treatment to PWMI
The NMHP faced issues related to coverage and provision of treatment to PWMI for several years. Mental disorders such as Substance Use Disorders (SUDs) and Child and Geriatric Psychiatric Disorders were excluded from the programme.4 Services were primarily curative and lacked preventive and promoted aspects.4
However, positive changes have been made by rolling out MNS services at HWCs under CPHC. The guidelines provide an implementation framework covering six groups of MNS disorders i.e. Common Mental Disorders (CMDs), Severe Mental Disorders (SMDs), Child and Adolescent Mental Health Disorders (C&AMHDs), Neurological Conditions, Substance Use Disorder (SUDs) and Suicide Ideation/Behaviors.16,17
Regardless of the advancements, important issues such as homelessness, participation of PWMI and caregivers in programme designing, implementation, and monitoring as well as patchy coverage of disability certification continue to require integration in the NMHP.12 The National Mental Health Policy, 2014 covers these issues explicitly, but its implementation needs to be monitored.
5. Way forward
NMHP has made considerable progress in the past few decades and is in different stages of implementation across the country with many desired modifications. Addressing the challenges for effective implementation will improve health outcomes nationally and globally.
Regarding governance, there is a need to extend psychiatric units at the subdistrict level and beyond for effective dissemination of mental health services. To provide ‘right care’ at the ‘right place’, services should be easily accessible, especially for individuals experiencing distress. Addressing the leadership and motivation issues with programme officials,5 training and incentivization are critical. While training and attitudinal orientation will facilitate effective service delivery, incentives will keep motivation high.
Efforts made towards community participation and IEC activities need to be continued while involving stakeholders, with focus on health communication followed by program communication. In addition to caregiver groups, user groups and Jan-Sansad, area influencers, gram panchayats and religious leaders should make concerted efforts to enable NMHP’s success on the community level. All IEC/BCC plans should be periodically monitored across all states.25
Issues such as homelessness, participation of PWMI and caregivers in programme designing, implementation, and monitoring as well as patchy coverage of disability certification must be dealt with in NMHP. With National Mental Health Policy, 2014 covering these issues explicitly, it is only reasonable that its implementation is monitored.
There is a need to mobilize additional HR for both preventive and curative strategies. HR where available, may be rationally deployed and responsibilities may be distributed carefully between genders to ensure effective screening, control and management of mental health diseases.20 While ASHAs may be trained to screen individuals for common mental health conditions,29 a new cadre of community mental health workers (CMHW) may also be created at the PHC level for screening and facilitating treatment as recommended by policymakers.4
The issues related to fund flow, utilization and accessibility must be resolved. Resource allocation of Rs 40 crore for the states and Rs 83.2 lakhs for DMHP for a total of 692 districts is insufficient, especially with the devastating impact of the COVID-19 pandemic on mental health. Additional funds may be mobilized to provide optimal health services aligning with NMHP goals to ensure availability and accessibility of minimum mental healthcare for the population. States must commit to their part of financial responsibility and ensure that implementation is coherent across districts. Inspiration may be taken from Kerala where funds and strong community support are enabled by elected representatives and funding sources that extend beyond the funds allocated by the government.25
Lastly, the absence of a robust monitoring system leaves no scope for evaluations and evidence generation that are essential for mid-course corrections. For that, evaluation of the activities under NMHP should be conducted periodically. Issues such as lack of central support and non-maintenance of the database need to be resolved.4 Connectivity issues in hard-to-reach areas, if any, must be fixed to enable a regular flow of information. The guidelines outlined by the central and state governments on periodic monitoring and evaluation need to be adhered to.
6. Conclusion
The NMHP has witnessed significant progress in terms of policy and programme development since its inception. However, challenges to effective implementation remain. Based on this review, factors such as fragmented governance, financial constraints, shortage of trained human resources, lack of a robust M & E mechanism, community participation and IEC/BCC related issues, and issues related to coverage and treatment of PWMI continue to adversely affect programme implementation. Though significant improvements concerning these issues have been made, some aspects continue to be desired. With the correct measures, NMHP has the potential to make a national and global impact on addressing the burden of mental health diseases.
Acknowledgements
NA