INTRODUCTION
The COVID-19 pandemic continues to evolve, causing important psychological repercussions in the general population, but especially in health professionals such as medical and nursing personnel in training, who continue to be in direct contact with the risk,1 and are subjected to excessive work demands with long working hours that are associated with frustration, family, and social isolation.2 Negative experiences can distort the perception of risk and evolve into a wide range of mental health problems,3 with depressive symptoms, anxiety, insomnia, and emotional distress being reported more frequently,4 as well as other prolonged maladaptive distress reactions, extreme fear of illness, anger, post-traumatic stress disorder, somatization, and high-risk behaviors. In addition, the pandemic has put doctors in an unprecedented situation, having to make challenging decisions and working under extreme pressure.3
In the case of Mexico, as in China, decisions include allocating scarce resources equally to patients who require it, providing care with insufficient resources, and giving bad news to the family. Furthermore, they struggle balancing their own physical and mental needs with the need to attend not only patients but relatives too, this distress increases when experiencing fear of contagion and spread of the virus to their family, even their friends or colleagues.5 At a global level, it has been reported that health professionals have been exposed to the constant threat of contagion by COVID-19, which causes a feeling of danger and constant uncertainty in their daily activities. In addition, exhaustion in these professionals by itself has been associated with anxiety, depression, and post-traumatic stress.6
Medical and nursing personnel in training are particularly vulnerable to mental health impact, with higher rates of psychological distress reported than in the general population. Factors that increase stress have been identified, such as exam preparation, the structure of medical programs, and academic schedules.7 The COVID-19 pandemic has generated a negative impact on mental health in health personnel in training due to the loss of interaction with their peers, absence from the family, social disconnection, financial stress, and general disruption of job functioning because of psychological anguish.8 Other studies have also reported high prevalence’s of depression, anxiety and stress in this population.9,10
As previously documented, the COVID-19 pandemic has a greater negative impact on the mental health of health personnel, therefore, it is necessary to identify these symptoms in order to provide specialized care in a timely manner and reduce integrity risks.
In this perspective, the hypothesis of this study is that military health personnel in training have a greater impact on their mental health, both because they experience the pandemic and because of the working conditions of medical training in the military. The present research aims to determine the prevalence of symptoms of depression, anxiety, and post-traumatic stress in professional health personnel in training, who have cared for patients with COVID-19 in a military setting.
METHODS
Study design
A cross-sectional study was conducted from March to September 2021.
Selection of participants was done through a non-probability convenience sampling, health professionals in training, doctors and nurses in a military center in Mexico City were selected. They were surveyed online.
Study sample consisted of medical staff and nursing staff enrolled in any medical specialty at the Military Graduate School of Health, who have cared for patients with COVID-19 during 2020 and signed an informed consent.
The sample size (n = 139) for a finite population (N = 280) was calculated with a confidence level of 95%, precision of 3% and a non-response rate of 15%, obtaining a calculation of n = 139 individuals.
n=N∗Z21−α/2∗p∗q/d2∗(N−1)+z21−α/2∗p∗q
Where: = sample size
= finite population size (in this case = 280)
= Confidence level (1.96)2
= prevalence of the characteristic of interest. Since this data is unknown, 50% (0.5) is noted
= : probability of not finding the characteristic (0.95)
= precision level (3%) and considering the adjustment for sample loss (15%).
Study variables
Independent variables: a) Sociodemographic variables: sex (0 = female, 1 = male); age (years), place of residence (entity where you live), religion (religious belief that you profess), marital status (0 = single, 1 = married or in a relationship); number of children, profession of health personnel (medicine = 1, nursing = 2); type of medical specialty (0 = invasive specialty, 1, non-invasive medical specialty); years of medical specialty (continuous numerical variable from 1 to 5 years relative to the year the participant is studying).
b) Variables of exposure to COVID-19: history in the year prior to the study of having 1) suffered from COVID-19, 2) a family member who suffered from the disease, and 3) a co-worker who became ill with COVID-19.
Dependent variables: Prevalence of depression (no depression = 0, mild depression = 1, moderate depression = 2, moderately severe depression = 3, and severe depression = 4). Prevalence of anxiety (no anxiety = 0, mild anxiety = 1, moderate anxiety = 2, and severe anxiety = 3). Prevalence of Post-Traumatic Stress Disorder -PTSD, (0 = absence and 1 = presence of PTSD.
Instruments
Scales validated in the country were applied to determine depression, anxiety, and post-traumatic stress.
Depression: The Patient Health Questionnaire-9 (PHQ-9) is an instrument validated in the Mexican population for the detection of depressive disorders. It establishes the diagnosis of depression through the DSM-IV criteria and determines the severity of said disorder. It can also be used to observe changes experienced by patients over time. It is made up of 9 items with a Likert-type response with values between 0 and 3 that refer to the last two weeks.11 For the Spanish version, results comparable to the original version were found, with sensitivity values of 87% and specificity of 88%.12
For its correction, a total score is obtained that ranges between 0 and 27. The proposed cut-off points are: 1-4 minimal depression; 5-9 mild depression; 10-14 moderate depression; 15-19 moderately severe depression; 20-27 severe depression.
Anxiety: The Generalized Anxiety Disorder Scale-7 (GAD-7) is designed to detect and measure the severity of generalized anxiety disorder, consists of 7 questions, with the following scores: 0 –4 no anxiety is appreciated; 5–9 mild anxiety symptoms are noted; 10–14 show moderate anxiety symptoms; 15–21 severe anxiety symptoms are noted.13
Stress: The Post Traumatic Stress Disorder Checklist (PCL-5) is a 20-item questionnaire, developed based on the diagnostic criteria proposed in the fifth version of the Manual Diagnosis and Statistics of Mental Disorders (DSM-5), which is evaluated by means of a Likert-type scale, ranging from 0 (nothing) to 4 (totally), these items describe the symptoms referring to the diagnostic criteria of re-experiencing, avoidance, activation and cognitive alterations. It is validated in the Mexican population with an internal consistency of (α =.97), as well as an appropriate convergent validity (rs = .58 to .88). The cut-off to establish post-traumatic stress is 33 points measured by PCL-5 scores, if total PCL-5 measurement ≥ 33 = PTSD).14
Procedure
With the help of experts in the field, the sociodemographic data collection questionnaire was constructed and captured in digital format, the items of each instrument used were also captured. The email addresses of the health personnel in training at the Military Graduate School of Health were requested from the academic section. The questionnaire was sent through the Survey Monkey platform to the different emails. Voluntary participation was requested through an online informed consent. If they did not agree to participate, the survey was automatically closed. The questionnaire consisted of mandatory answers to move on to the next question. If they did not complete the questionnaire, such data was deleted; only completed questionnaires were considered. The surveys were saved in the online database as they were recorded. Data was exported from Survey Monkey to SPSS v.26 statistical software for analysis, (IBM Corp).
Statistical analysis
A descriptive analysis was performed by obtaining the absolute and relative frequencies of the categorical variables in addition to the respective percentages. The prevalence’s of depression, anxiety and PTSD were determined. For numerical variables, the means were described with their standard deviation. Bivariate analyzes were performed with Chi2 tests or t-tests according to the variables, comparing the independent variables described with the presence of symptoms of depression, anxiety and/or PTSD.
For the inferential analysis, a Binary Logistic Regression method was applied and subsequently a Multiple Logistic Regression, contrasting the significant independent study variables associated with the presence of PTSD.
In addition, a Pearson Correlation was performed, looking for correlations between the study variables and the total PCL-5 scores. Pearson’s correlation coefficient ranges from –1 to +1: a value less than 0 indicates a negative and inverse correlation. A value greater than 0 indicates that there is a positive correlation. Pearson’s correlation coefficient (r) was used as an inferential statistic (to test whether the relationship was significant), r was reported alongside its P-value. Statistical significance was set at P<0.05.
RESULTS
Sociodemographic characteristics of the sample
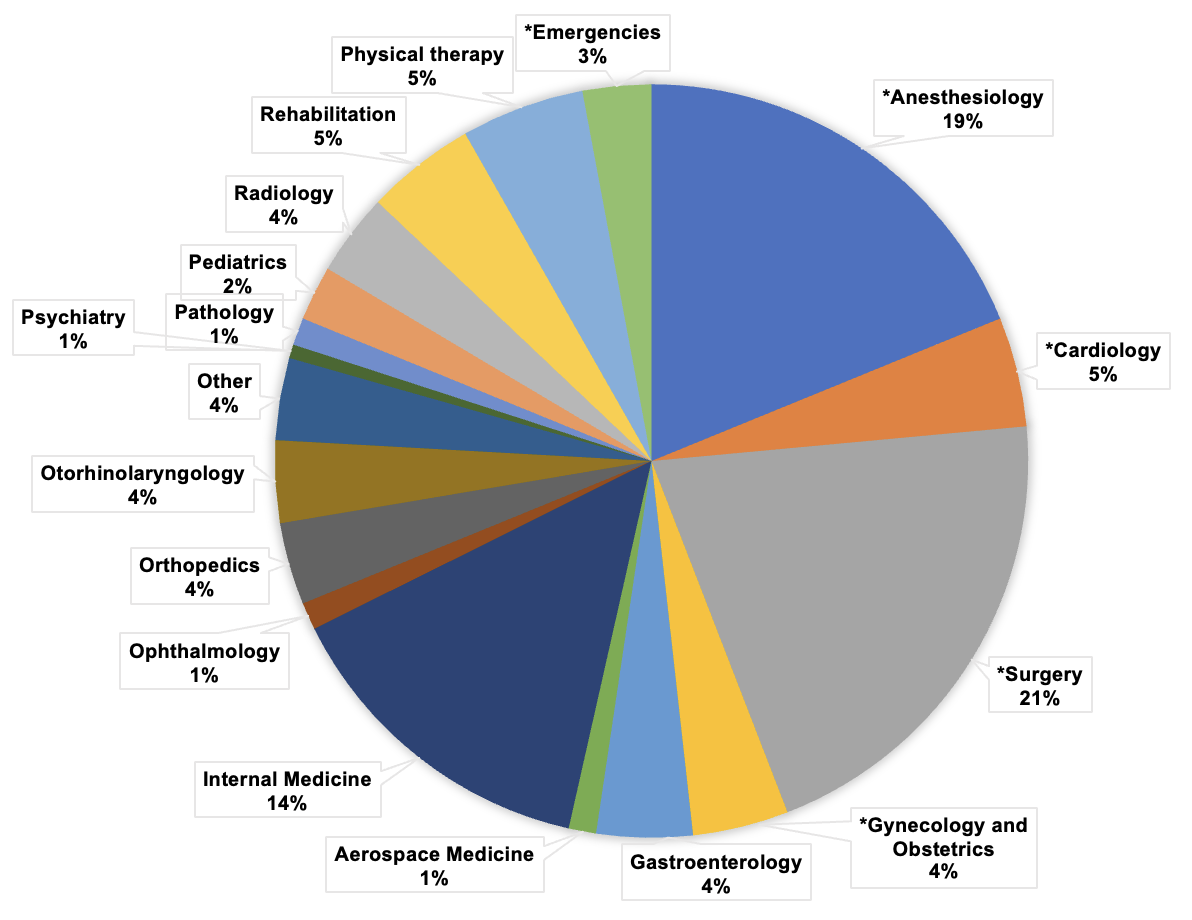
A total of 170 military health personnel in training residing in Mexico City were surveyed online; 54% (n = 91) corresponded to the female sex, 52% of the participants were in the age group between 30 and 39 years, most of them with single marital status (59%; n = 101) and without children (64%; n = 64%), 16% lived alone (n = 27); 76% stated that they were Catholic (n = 129). Of the participating health personnel, 76% (n = 129) reported being a physician and 24% (n = 41) were nursing personnel. The type of medical specialty of the health personnel surveyed is shown in Figure 1.

Characteristics of exposure to COVID-19
Among the health personnel, 39% (n = 66) reported having suffered from COVID-19 during 2020, 3% (n = 5) of them suffered more than one infection. Of the sample, 64% (n = 109) stated that they had a close relative who suffered from COVID-19 during the same year, and more than 89% (n = 152) reported having a co-worker who suffered from COVID-19 during 2020. The health personnel in training, considered to be the front line in the care of COVID-19 at the Central Military Hospital, mentioned attending an average of 14 patients (per day) with COVID-19 in a work week, but 30% of the participants (n= 51) reported treating an average of 30 patients (per day) in a work week.
Clinical characteristics in the study sample
Depressive symptoms
It was found that 34% (n = 57) of the study sample presented mild to severe depressive symptoms, many of the participants (23%) were found to have mild symptoms, 7% had moderate symptoms, 3% had moderate severe symptoms and 1.2% reported severe symptoms.
Anxiety symptoms
Only 30% (n = 51) of the participants reported anxiety symptoms, of which 19% reported mild anxiety symptoms, 7.1% reported moderate anxiety symptoms, and 4% severe anxiety symptoms.
Symptomatic dimensions of post-traumatic stress
Of the participants, 39% (n = 66) manifested symptoms of post-traumatic stress, with symptoms within the activation dimension being more prevalent 11.24% and cognitive alterations 11%). But the mean scores and standard deviation (SD) for each dimension of the PCL-5 scale were: 1) Total PCL = 7.98, SD = 13; 2) PCL-Avoidance-Amnesia = 1.02, SD = 2.1; 3) PCL-Cognitive Alterations = 2.58, SD = 4.39; and 4) PCL-Reexperiencing = 1.65, SD = 3.14
Comparisons between male and female participants groups
Considering the previous descriptive results, comparisons of the qualitative study variables were made with respect to sex, finding that single marital status predominates in females compared to males (36% vs 24%, X2 = 4.72; P < .05). Other relevant associations are shown in the profession variable, in medical professionals the male sex prevails, while in nursing, the female sex predominates (X2 = 15.79; P < .001). With marginal significance is the fact of having children or not, observing that women without children predominate compared to men (37.1% vs 26.5%).
Regarding the exposure to COVID-19, a significant difference was only found between the sexes in relation to the history of a relative who suffered from COVID-19. Table 1.
Although 39% of the total study sample manifested some symptom of post-traumatic stress in one or more dimensions, only 6 % qualified in the PCL-5 Total ≥ 33, that is, as a probable post-traumatic stress disorder. Regarding the sociodemographic variables and the measurement of the total PCL-5 ≥ 33, only statistically significant differences were found in marital status by sex. See Table 2. The PHQ-9 scores by level show that the participants who manifested symptoms of depression also expressed post-traumatic stress symptoms, an association that was found to be significant for cases of severe depression T = 49.80, SD = 8.25; P < .001).
Association between clinical variables
With respect to the variables of exposure to COVID-19, a significant association was only found if a relative became ill with COVID-19 and total PCL-5 (F = 8.26; P < .001).
In the clinical variables, we found significant associations between presence of anxiety, measured through the GAD-7 scale, and the total PCL-5 (Mean = 11.74, SE 1.16; P < .001). Similarly, we observed associations between the presence of depression, measured through the PHQ-9, and the PCL-5 scores (Mean = 9.64, SE 1.30; P < .001).
Logistic Regression (LR) models were made to adjust the study variables with dichotomous categories (dummy variables), prior to performing a Multiple Logistic Regression.
PHQ-9 and PCL-5: Model fit: Introduce method, R2 = 56%, adjusted R = 56% and Standard Error = 8.6, a total PHQ-9 score increased the total PCL-5 score by 2.12, association with a very robust value of the test F = 216.5 and P < .001.
GAD-7 and PCL-5: Model fit: Introduce method, R2 = 66%, adjusted R = 66% and Standard Error = 7.5, a total GAD-7 score increased the total PCL-5 score by 2.35, association with a very robust value of the F test = 333.9 and a P < .001.
Multiple Logistic Regression
With the one-step input method, the LR model with the best fit was chosen according to the omnibus test of model coefficients: Chi-squared = 42.647, df = 4 and significance < .001; with Cox and Snell’s R squared =.222 and Nagelkerke’s R2 = 615; which indicates that the model explains more than 22% of variability in the response variable or PTSD. When all previously significant study variables in the binary LR or predictors (sex, relative infected with COVID-19 in the last year, co-worker infected with COVID-19 in the last year, and scores of PHQ-9 and GAD-7) were introduced, it is observed that PHQ-9 and GAD-7 maintain their significant association. See Table 3.
Pearson’s correlation (Coefficient r)
The findings show that variables associated with total PCL-5, were the history of having a relative infected with COVID-19, and total PHQ-9 and GAD-7 scores. It is relevant to mention that all the variables shown in Table 4 are significantly associated with the total score of the PCL-5, in some associations a Pearson correlation coefficient was observed with small values, this is because said coefficient measures the linear relationship, and small values indicate that the association is non-linear. See significance in Table 4.
DISCUSSION
The results of this study confirm that health personnel in training, doctors and nurses in the military, show higher prevalence than other health workers of post-traumatic stress symptoms with 39%, depression with 34% and of anxiety with 30%. It was also shown that 6% of the study sample presented severe forms of mental impairment, such as post-traumatic stress disorder. The data from this first study in Mexico, reports mental health involvement in health professionals in training in a military setting, data consistent with the international literature.15,16 The psychological impact of COVID-19, with the presence of common mental illnesses such as post-traumatic stress, anxiety, and depression, represents an important challenge, since professional health personnel in training in Mexico make up a large part of the workforce in specialized health care services, and in turn, represent the first line in the fight to mitigate the pandemic.17 Still, they are frequently subjected to heavy workloads with long working hours resulting in negative repercussions on their long-term mental health.2,15 In fact, it has been reported that during the first wave of the COVID-19 pandemic, certain institutional conditions such as strict biosafety requirements, the discomfort of protective equipment, the lack of sufficient equipment, isolation in specific areas for the care of patients with COVID-19, the feeling of injustice around the distribution of work by services, among other factors, increased the prevalence of stress in medical residents.18,19 Our findings showed a higher prevalence of post-traumatic stress symptoms in health personnel in training who practice invasive specialties, such as anesthesiology and surgery, which require the use of more sophisticated equipment; this is a similar finding to that reported in another study.20
Another relevant result among the participating military health personnel professionals in training is that a higher prevalence of mental symptoms was observed in female personnel, single, aged between 30 and 39 years, and with family members sick with COVID-19, similar data to other international studies.21,22 In the military field, the findings can be explained seeing that resident doctors in the front line of patient care are allowed to continue their professional development, but professionals at older ages are not as able to enter the field, the demands of the career postpone marriage and the formation of a family.
The prevalence of anxiety and depression in the health professionals in training participating in our study were similar to those reported in the literature,16 the same did not occur with the prevalence of 6% shown for post-traumatic stress, which was lower than that found in other studies.23,24 In addition, our study showed that male and married staff were the most affected by PTSD, although the civil status is consistent with what was reported, it does contrast for sex, a possible explanation is that 90% of its study sample was made up of females.24 We did not find antecedents in the literature that explain the higher prevalence of PTSD in married men within the professional military personnel in training, we infer that the military population presents symptoms of stress when constantly changing place of residence and having to temporarily abandon the family, as well as presenting fear, anxiety, and stress at the risk of contracting the virus and infecting their partner. We identified that military health professionals in training presented greater post-traumatic stress symptoms associated with having a family member infected with COVID-19, this due to family idiosyncrasies in the Mexican context, since it is this that provides emotional, social, and psychological support.25 Health professionals in training, on the other hand, are particularly vulnerable to poor mental well-being and have higher rates of psychological distress compared to the general population.26 Several factors have been reported to contribute to stress in medical students, including academic factors such as feeling unprepared for exams; the organizational structure of medical courses and schedules,7 as well as personal psychosocial resources, which are factors that have intrinsic value or are useful in pursuing goals and coping with demands and confronting the stress of everyday life.27
One of the limitations of this study was that participants were invited to the study virtually, which may discourage the willingness of them to enroll in the study. Despite having a 61% participation rate (out of a total of 280 potential individuals), the small sample size did not allow more complex analyzes to be carried out. Nonetheless, the authors believe that this is a pioneering study in Mexico that provides valuable information to be considered in mental healthcare strategies in military health personnel in training and preventing long-term problems.
In conclusion, our findings, show that the military medical professionals are the ones that have the greatest affectation of mental health, manifesting the most prevalent common ailments such as post-traumatic stress symptoms, anxiety, and depression, and that working hours, work pressure, fear of contagion and the need to make decisions have a decisive impact on people’s lives, especially those professionals who work in intensive care units. If these conditions are not treated, they can generate post-traumatic stress symptoms and evolve into severe conditions such as PTSD in the long term. Although stress is a natural response to the threat of the COVID-19 pandemic, the conditions of health institutions make military health professionals in training a vulnerable sector of society.
Therefore, we emphasize the need to carry out health promotion activities and preventive actions in military health personnel in training such as routine screening, and continuously provide comprehensive health care activities to improve the quality of life of these professionals, and consecutively, improve the quality of patient care.
Ethical considerations
In order to comply with the ethical aspects of research in human beings, the study protocol was approved by the Ethics Committee of the Military Graduate School of Health. Register: FMSPUM-04-22.
Financing
None.
Conflict of interests
The authors declare they have no conflicts of interest.
Acknowledgements
The authors thank the Master’s Program in Public Health of the Military Graduate School of Health (Secretaría de la Defensa Nacional, México), for the facilities to develop this research.